Printable Dental Claim Form
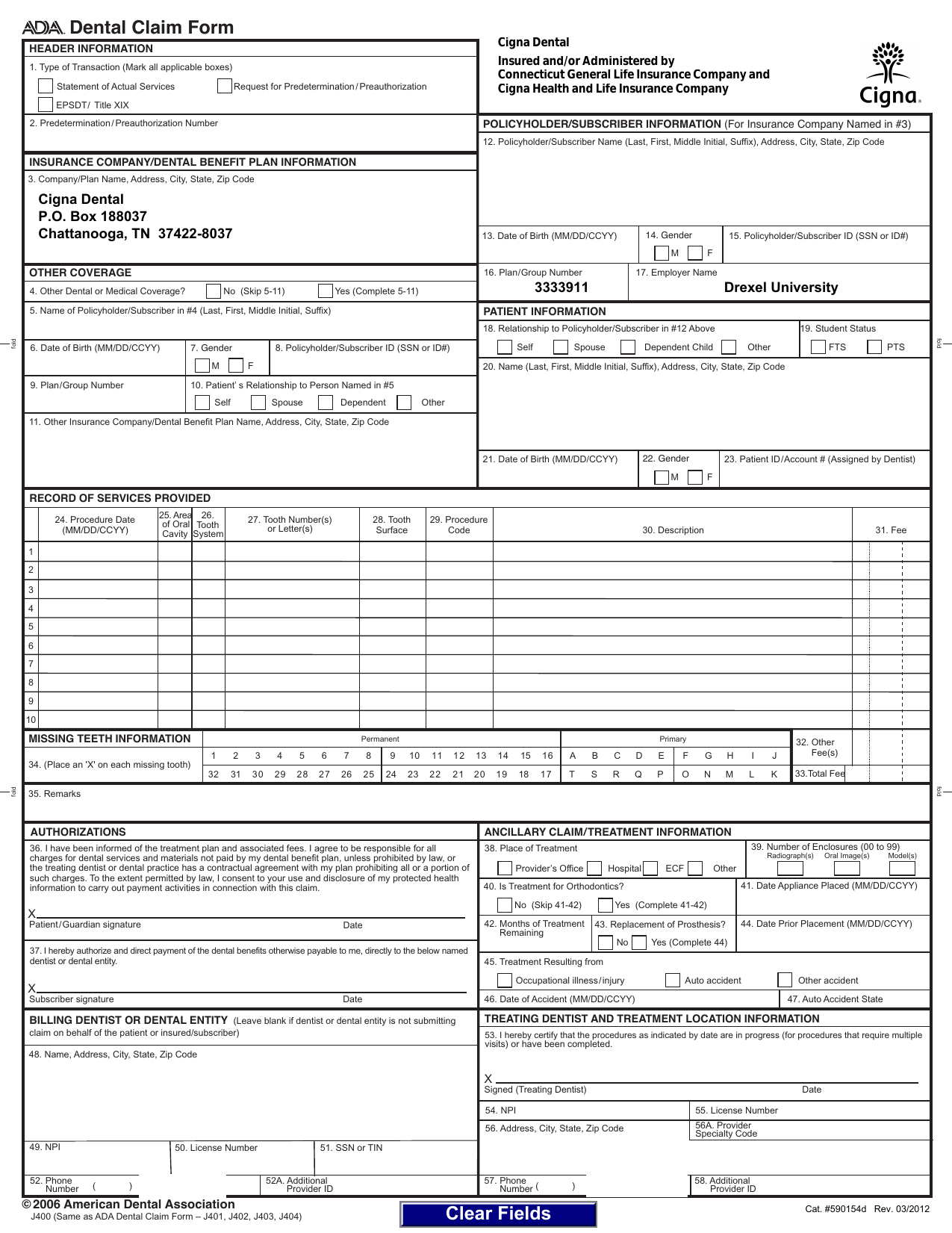
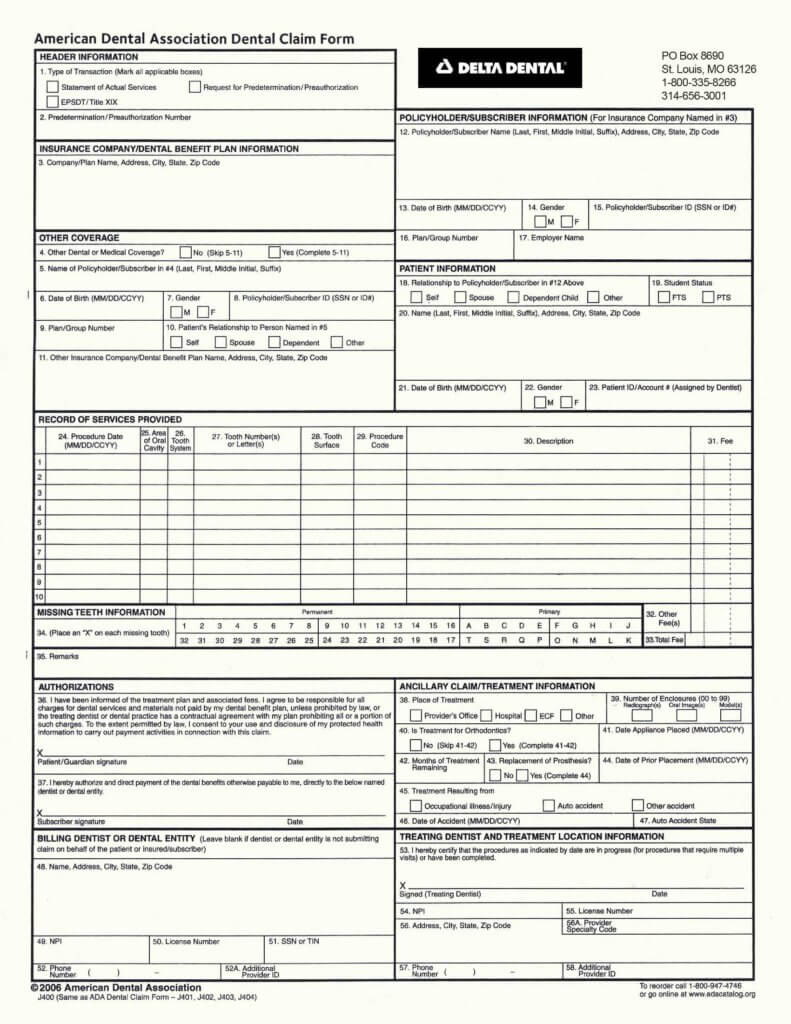
Printable Dental Claim Form - For any questions regarding pricing or purchasing. The following information highlights certain form completion. The ada dental claim form was revised for 2024 with editorial changes, additional fields to document treatment. Web to reorder call 800.947.4746 or go online at adacatalog.org. Web for information about licensing of the ada dental claim form, please see cdt. Web the ada dental claim form was last structurally revised in 2012 to incorporate key data content changes that enables. Web dental claim form type of transaction (mark all applicable boxes) request for predetermination/preauthorization. Policyholder/subscriber name (last, first, middle initial, sufix), address, city, state, zip code 13. Web dental claim form type of transaction (mark all applicable boxes) statement of actual services request for.
Delta Dental Printable Claim Form Printable Forms Free Online
Dental Claim Form 20132021 Fill and Sign Printable Template Online

Free Printable Ada Dental Claim Form Printable Templates
Fillable Dental Claim Form Printable Forms Free Online
Printable Dental Claim Form 2018 Fill and Sign Printable Template
Fillable Dental Claim Form Printable Forms Free Online
Dental Claim Form printable pdf download
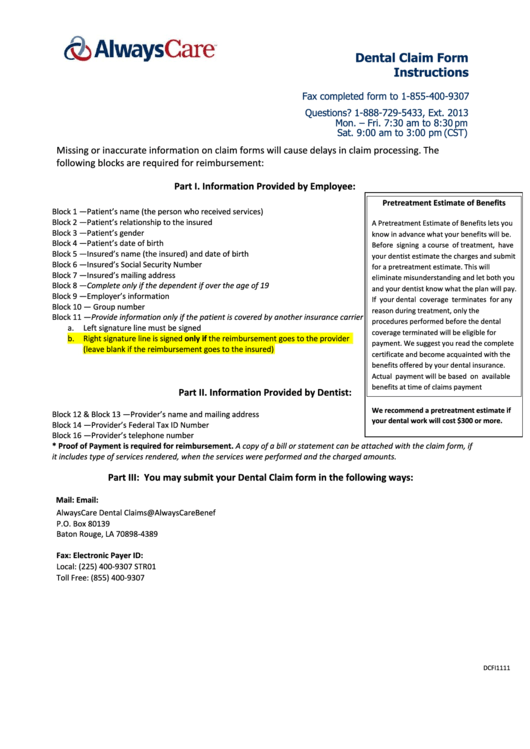
Fillable Form F54288a Dental Care Claim Form printable pdf download
Delta Dental Printable Claim Form Printable Forms Free Online
Fillable Standard Dental Claim Form Groupsource printable pdf download
The Ada Dental Claim Form Was Revised For 2024 With Editorial Changes, Additional Fields To Document Treatment.
Web for information about licensing of the ada dental claim form, please see cdt. Web dental claim form type of transaction (mark all applicable boxes) statement of actual services request for. Web dental claim form type of transaction (mark all applicable boxes) request for predetermination/preauthorization. For any questions regarding pricing or purchasing.
The Following Information Highlights Certain Form Completion.
Web the ada dental claim form was last structurally revised in 2012 to incorporate key data content changes that enables. Web to reorder call 800.947.4746 or go online at adacatalog.org. Policyholder/subscriber name (last, first, middle initial, sufix), address, city, state, zip code 13.